About Impingement Syndrome

The shoulder joint is a complex structure that allows for a very large range of motion, but has very little stability. This makes the shoulder a common site of injury. The shoulder girdle is comprised of three bones; the humerus (upper arm), the scapula (shoulder blade), and the clavicle (collarbone). The scapula contains a bony protrusion called the acromion process, which allows it to connect to the cavicle. The humerus is connected to the scapula by the rotator cuff, which consists of four muscle tendons. Impingement syndrome is a painful shoulder condition that occurs when the tendons of the rotator cuff rub against the acromion pro cess. This rubbing or “impinging” action can cause inflammation of the bursa overlying the rotator cuff, or of the tendons themselves, and results in pain and limited range of motion at the shoulder.
cess. This rubbing or “impinging” action can cause inflammation of the bursa overlying the rotator cuff, or of the tendons themselves, and results in pain and limited range of motion at the shoulder.
 cess. This rubbing or “impinging” action can cause inflammation of the bursa overlying the rotator cuff, or of the tendons themselves, and results in pain and limited range of motion at the shoulder.
cess. This rubbing or “impinging” action can cause inflammation of the bursa overlying the rotator cuff, or of the tendons themselves, and results in pain and limited range of motion at the shoulder. Typical symptoms of impingement syndrome include a generalized minor pain in the shoulder, even during rest, as well as sudden pain with lifting and reaching movements. One characteristic sign of impingement is a sharp pain when the individual reaches for his or her back pocket. As the condition progresses, discomfort increases. The joint may become stiff, and overhead athletes may have a very difficult time completing the tasks required in their respective sports.
Risk Factors
- Repetitive Overhead Motions: The primary risk factor for impingement syndrome is involvement in activities that require excessive repetitive overhead motions. The force of these movements can cause attrition in the rotator cuff tendons. This occurs in sports such as tennis, throwing, and swimming, and is also common in certain occupations, such as carpentry.
- Weak or Inflexible Rotator Cuff Muscles: The four muscles of the rotator cuff are the supraspinatus, infraspinatus, teres minor, and subscapularis. These muscles perform abduction, external rotation, internal rotation, and horizontal abduction. If these muscles lack strength and flexibility, added force is likely to irritate the tendon at the rotator cuff and can lead to symptoms of impingement.
- Age: Though impingement syndrome can occur at any age, it is more common in young athletes and middle-aged people. Younger patients tend to recover more easily, whereas older patients are more likely to require surgical treatment.
Treatment
- Rest: The first step with nearly any overuse injury is to take a break from the activities that cause painful symptoms. Unfortunately, for athletes this may mean some time off from their sport. If possible, activities can be modified so that the humerus is kept below 70 degrees of abduction. This is done to protect the bursa and the rotator cuff tendons from further irritation due to impingement.
- Ice and Anti-Inflammatory Treatment: Pain and inflammation can be treated conservatively with ice and over the counter nonsteroidal anti-inflammatory drugs such as ibuprofen or naproxen. These treatments should be applied consistently, but within moderation. Ice should not be applied for longer than 15 to 20 minutes at a time, and anti-inflammatory medications should not be taken for extended periods of time as they may result in adverse side effects. If these basic anti-inflammatory procedures do not work, a doctor might suggest a cortisone injection for a temporary, but strong, anti-inflammatory effect.
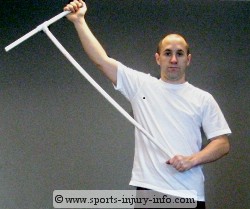 |
| AAROM Excercise for Shoulder Abduction |
- Physical Therapy: Physical therapy for impingement syndrome aims to reduce pain and inflammation, while reestablishing full range of motion at the shoulder joint. This is often accomplished by a combination of ice and heat therapy, isometric strengthening exercises in all of the muscles of the shoulder (not just the four rotator cuff muscles), active-assistive range of motion (AAROM) exercises, and sometimes neuromuscular control exercises. This could include transcutaneous electrical nerve stimulation (TENS), ultrasound, and iontophoresis, as well as several others. Physical therapy can be very effective, as long as the patient is consistent with his or her home exercises, and follows orders on what movements should remain limited.
- Surgery: In the rare event that 3 to 6 months of the above conservative treatments have not improved symptoms, surgery may be required to treat impingement syndrome. The goal of surgical treatment is to increase the space between the rotator cuff tendons and the acromion process, allowing the head of the humerus to move freely in the subacromial space. This act of relieving pressure from the subacromial tissues is referred to as subacromial decompression, and is usually performed by removing part of, and reshaping the acromion. This is also known as acriomioplasty. Surgery for impingement syndrome can be performed openly or arthorsocpically, depending on the case and the preferences of the surgeon. Rehabilitation, usually in the form of physical therapy, is required after surgery. This can be a long process, as this surgery may take a while to recover from.
An Ounce of Prevention
For overhead athletes and workers who may be at a high risk of impingement syndrome, several preventative measures can be taken. Instruction on proper warm-up techniques and strengthening exercises may help decrease the risk of shoulder injury. These individuals should also be aware of the early signs of impingement syndrome, so that early conservative treatment can be applied before the condition has a chance to progress to the point of inability to complete daily tasks.
Sources and Additional InformationAmerican Academy of Orthopaedic Surgeons http://orthoinfo.aaos.org/
http://emedicine.medscape.com/article/92974-overview
Lippert, Clinical Kinesiology and Anatomy, 4th edition
http://emedicine.medscape.com/article/92974-overview
Lippert, Clinical Kinesiology and Anatomy, 4th edition