 About Compartment Syndrome
About Compartment SyndromeCompartment syndrome refers to a painful condition in which the pressure within a group of muscles rises to potentially dangerous levels. Compartment syndrome can occur in several locations within the body, and may be categorized as either acute or chronic. Acute compartment syndrome usually develops as the result of a serious injury, and is classified as a medical emergency. Without immediate treatment, it can result in permanent muscle damage. Chronic compartment syndrome, also known as exertional compartment syndrome, generally occurs as an overuse injury. This overview will focus on compartment syndrome of the lower extremity, a condition that arises most commonly among athletes such as long-distance runners, skiers, basketball players, and soccer players.
 The lower leg is divided into four compartments; anterior, lateral, posterior, and deep posterior. Each of these compartments contains several muscles, along with corresponding nervous tissue and blood vessels. The compartments are separated by fascia (thick layers of tissue) that to not stretch or expand easily. Therefore, when swelling occurs within a compartment, increased pressure can be placed on the muscles, capillaries and nerves. In the case of chronic compartment syndrome, this results in pain, cramping, tingling and/or numbness during activities such as running. These sensations tend to go away once the activity has stopped, though the muscles in the area of the symptoms may feel tight.
The lower leg is divided into four compartments; anterior, lateral, posterior, and deep posterior. Each of these compartments contains several muscles, along with corresponding nervous tissue and blood vessels. The compartments are separated by fascia (thick layers of tissue) that to not stretch or expand easily. Therefore, when swelling occurs within a compartment, increased pressure can be placed on the muscles, capillaries and nerves. In the case of chronic compartment syndrome, this results in pain, cramping, tingling and/or numbness during activities such as running. These sensations tend to go away once the activity has stopped, though the muscles in the area of the symptoms may feel tight. Chronic compartment syndrome of the lower extremity most commonly occurs in the anterior compartment, which houses the dorsiflexors of the foot and ankle (tibialis anterior, extensor digitorum longus, extensor hallucis longus, and peroneus tertius) as well as the anterior tibial artery and the deep peroneal nerve. This simply means that the characteristic symptoms of compartment syndrome are usually experienced in the front of the lower leg. Chronic compartment syndrome usually occurs bilaterally, meaning that symptoms are present in both legs.
Risk Factors
The only true risk factor for chronic or exertional compartment syndrome is participation in activities that involve repetitive motions. This condition is most commonly found in long-distance runners, but other sports listed as risk factors include cycling, soccer, and gymnastics. Chronic compartment syndrome most frequently occurs in athletes under the age of 40, though age is not considered to be a risk factor.
Treatment
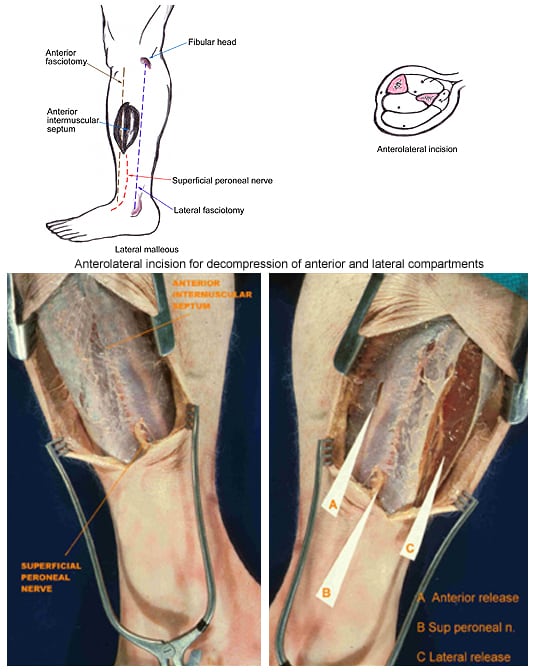 - Surgery: Unfortunately, surgical procedures seem to be the most effective treatment for chronic compartment syndrome. The most common surgery for compartment syndrome is a fasciotomy, or compartment release, which involves cutting the fascia to allow the muscle swell, and subsequently relieving the excess pressure. There are several techniques for performing this surgery, though the most common is the double-incision fasciotomy (shown on right). Rehabilitation is required after surgery, so compartment syndrome patients (especially athletes) should anticipate a fairly long recovery time before returning to normal activity.
- Surgery: Unfortunately, surgical procedures seem to be the most effective treatment for chronic compartment syndrome. The most common surgery for compartment syndrome is a fasciotomy, or compartment release, which involves cutting the fascia to allow the muscle swell, and subsequently relieving the excess pressure. There are several techniques for performing this surgery, though the most common is the double-incision fasciotomy (shown on right). Rehabilitation is required after surgery, so compartment syndrome patients (especially athletes) should anticipate a fairly long recovery time before returning to normal activity.- Non-Surgical Treatments: Chronic compartment syndrome may be treated conservatively; however, these treatments have not proven to be extremely effective in relieving symptoms over the long term. Pain medications, stretching and strengthening regimens, and biomechanical corrections (such as orthotics) are often used to delay the need for surgery. Generally speaking, if an athlete wishes to continue with the sport that caused the injury, he or she will most likely need surgery in order to return to full ability.
An Ounce of Prevention
Unfortunately, very little can be done to prevent the onset of compartment syndrome. General suggestions for reducing any chronic overuse injury include proper warm-ups and cool-downs with exercise, gradual approaches to increased training, proper footwear, and running on a variety of surfaces.
Sources and Additional InformationAmerican Academy of Orthopaedic Surgeons http://orthoinfo.aaos.org/topic.cfm?topic=a00204
Mayo Clinic http://www.mayoclinic.com/health
http://emedicine.medscape.com/article/1270542-treatment
Lippert, Clinical Kinesiology and Anatomy, 4th edition
Sources and Additional InformationAmerican Academy of Orthopaedic Surgeons http://orthoinfo.aaos.org/topic.cfm?topic=a00204
Mayo Clinic http://www.mayoclinic.com/health
http://emedicine.medscape.com/article/1270542-treatment
Lippert, Clinical Kinesiology and Anatomy, 4th edition