About Plantar Fasciitis
About Plantar FasciitisThe plantar fascia (or plantar aponeurosis) is a dense connective tissue structure, similar to a tendon or ligament, which extends along the bottom of the foot. It consists of three bands (medial, central, and lateral) and runs from the calcaneus (heel bone) to the heads of the metatarsals and proximal phalanges (ball of foot), providing a strong mechanical linkage between these structures. The plantar fascia plays an integral role in maintaining the medial longitudinal arch and increasing the stability of the foot during weight-bearing activities.
 Plantar fasciitis refers to a condition typically resulting in pain near the origin of the plantar fascia, on the underside of the foot, just in front of the heel. Patients often report the pain being at its worst first thing in the morning, decreasing throughout the day while walking around. This plantar pain often returns near the end of the day if the individual spends a lot of time on his or her feet.
Plantar fasciitis refers to a condition typically resulting in pain near the origin of the plantar fascia, on the underside of the foot, just in front of the heel. Patients often report the pain being at its worst first thing in the morning, decreasing throughout the day while walking around. This plantar pain often returns near the end of the day if the individual spends a lot of time on his or her feet. The suffix “-itis” generally indicates a condition of inflammation, though some histological studies have reported an absence of inflammatory infiltrate in plantar fasciitis patients. These studies have linked plantar fasciitis with more degenerative changes in the plantar fascia, such as collagen degeneration, micro tears and calcification, especially in older patients. Whatever the exact cause may be, plantar fasciitis can be very painful and limits the lifestyles of many active individuals.
Risk Factors
Plantar fasciitis is a fairly common overuse injury that affects more than two million Americans each year. Any combination of certain risk factors significantly increases an individual’s chance of developing this painful condition.
- Gender: Women are more likely to develop plantar fasciitis than men.
- Age: Plantar fasciitis can occur at any age, though most commonly reported in patients between the ages of 40 and 60.
- Weight: Overweight and obese individuals are more likely to develop plantar fasciitis, due to the strain that extra weight places on the plantar fascia.
- Lifestyle and Activity Level: Plantar fasciitis has a much higher incidence in individuals that spend a considerable amount of time on their feet, especially on hard surfaces. Waiters/waitresses, teachers, and factory workers are common sufferers of plantar fasciitis. Additionally, athletes who regularly participate in high-impact activities, such as jumpers, dancers, and long-distance runners are at an increased risk.
- Foot Mechanics: Plantar fasciitis is linked to several variations in foot structure and gait patterns. Individuals with very low or very high arches tend to be at a higher risk for this injury. Low arches can put stress on the plantar fascia by forcing it through excess motion, and are correlated with overpronation (or “rolling in”) of the foot during weight-bearing. This causes an overstretch of the plantar fascia which can lead to the characteristic pain of plantar fasciitis. High arches, on the other hand, can lead to plantar pain as a result of the foot’s inability to dissipate force. The tightness and rigidity found in a high-arched foot often lead to underpronation, sometimes referred to supination (or “rolling out”) of the foot during weight-bearing. Many other biomechanical aspects of the foot, as they related to plantar fasciitis, are still being studied. Some studies also suggest that a limited range of ankle dorsiflexion and tight Achilles tendons are associated with a higher risk of plantar fasciitis.
- Improper Footwear: Spending significant amounts of time in improper footwear can be a major risk contributor, especially for those who are already predisposed to plantar fasciitis by one of the aforementioned factors. Flip-flops, ballet flats, and other shoes with thin soles and little arch support should be worn in moderation, as they can lead to flattening of the foot and excess strain on the plantar fascia. High heels can cause the Achilles tendon to contract and shorten and should also not be worn for extended periods of weight-bearing.
As far as athletic footwear, individuals with low arches, or those who overpronate, should look for shoes marked as “stability” or in more severe cases “motion control.” These shoes incorporate a more rigid material along the medial longitudinal arch of the foot to help prevent the foot from rolling in excessively. Athletes with high arches, or those who underpronate, should select shoes with higher cushioning and less rigid stability. Proper footwear selection is critical for athletes such as cross country runners, who spend great amounts of time doing repetitive weight-bearing activity. These should be replaced every 300-500 miles.
Treatment
The extensiveness of the treatment required to improve plantar fasciitis symptoms varies greatly among individual cases. For some patients, taking a few weeks off from activities (i.e. jumping, running) that put excessive strain on the heel is enough of a remedy.
- Pain and Inflammation Relief: Though debate remains as to whether or not plantar fasciitis is an inflammatory condition, many patients find that ice and anti-inflammatory drugs (such as ibuprofen, aspirin, or naproxen) help to relieve symptoms. Ice should be applied several times a day, usually after periods of weight-bearing or strenuous activity. Duration of each ice application should not exceed 20 minutes.
- Structural Support: Some patients choose to wear specially designed splints at night, which hold the foot in a slightly dorsiflexed position during sleep. This stretches the plantar fascia and can help to relieve morning pain. During the day, selection of proper footwear is critical (see above). Those inflicted by plantar fasciitis might consider being fitted for the right shoe at a running store. Other structural options include the insertion of orthotic devices into old shoes. Heel inserts are available at most drugstores, and have been shown to decrease impact on the heel. Plantar fasciitis patients should never go barefoot.
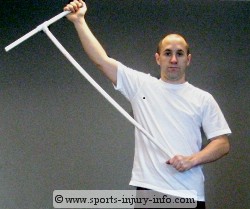
 - Stretching: Gentle stretching of the plantar fascia has proven to be an effective way of restoring flexibility and reducing pain. There are a number of different ways to do this, but most involve variations of dorsiflexion in the foot. Simple stretching programs can be designed by physical therapists, athletic trainers, etc. and most often include stretching of the calf muscles, Achilles tendon, and of the plantar fascia itself. The ProStretch is a common device used for stretching the fascia.
- Stretching: Gentle stretching of the plantar fascia has proven to be an effective way of restoring flexibility and reducing pain. There are a number of different ways to do this, but most involve variations of dorsiflexion in the foot. Simple stretching programs can be designed by physical therapists, athletic trainers, etc. and most often include stretching of the calf muscles, Achilles tendon, and of the plantar fascia itself. The ProStretch is a common device used for stretching the fascia.  - Strengthening: Physical therapy is often very beneficial to plantar fasciitis patients and consists of a series of stretches and strengthening exercises. Strengthening exercises are often focused on the intrinsic muscles of the foot (muscles with origins and insertions both within the foot itself). These exercises include toe curls with a towel and toe taps. If the cause of the plantar fasciitis symptoms is linked to overpronation or underpronation that can be attributed to a muscle weakness somewhere else in the leg, these muscles are also treated with strengthening routines.
- Strengthening: Physical therapy is often very beneficial to plantar fasciitis patients and consists of a series of stretches and strengthening exercises. Strengthening exercises are often focused on the intrinsic muscles of the foot (muscles with origins and insertions both within the foot itself). These exercises include toe curls with a towel and toe taps. If the cause of the plantar fasciitis symptoms is linked to overpronation or underpronation that can be attributed to a muscle weakness somewhere else in the leg, these muscles are also treated with strengthening routines.- Injections: Sometimes, in the case of chronic or reoccurring plantar fasciitis, a patient will elect to try corticosteroid injections for pain relief. These injections have proven to be about 70 percent effective, but are associated with a risk of rupturing the plantar fascia entirely. It is for this reason that injections are often reserved for instances where other treatments are ineffective.
- Surgery: In rare instances (5-10% of cases) where the individual does not respond to any of the more conservative forms of treatment, he or she may consider surgical release of the plantar fascia (plantar fasciotomy). This surgery has been reported to have a 70 to 90 percent effectiveness rate, but like all surgeries, is associated with some risk.
An Ounce of Prevention
As with any overuse injury, prevention methods are the most effective way to avoid chronic plantar pain. Though the wide array of risk factors associated with plantar fasciitis predisposes a large population, many of these risk factors can be counteracted.
For obese and overweight individuals, the best way to prevent plantar fasciitis (as well as many other conditions and injuries) is to lose weight. For people who work in environments or lead lifestyles that require a great deal of standing and walking, proper footwear is essential. Athletes, especially those participating in high-impact sports, should take extra caution to be sure they are wearing a shoe that corresponds with their foot type (see above). Stretching and strengthening routines can easily be performed at home to prevent injury and the necessity for physical therapy. Remember, overuse injuries are much easier to prevent than they are to cure!
Sources and Additional Information
Journal of Athletic Training
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC385265/
American Academy of Family Physicians
http://www.aafp.org/afp/2001/0201/p467.html
Mayo Clinic
http://www.mayoclinic.com/
Harvard Women's Health Watch
http://www.health.harvard.edu/
Lippert, Clinical Kinesiology and Anatomy, 4th Edition.
 About Compartment Syndrome
About Compartment Syndrome The lower leg is divided into four compartments; anterior, lateral, posterior, and deep posterior. Each of these compartments contains several muscles, along with corresponding nervous tissue and blood vessels. The compartments are separated by fascia (thick layers of tissue) that to not stretch or expand easily. Therefore, when swelling occurs within a compartment, increased pressure can be placed on the muscles, capillaries and nerves. In the case of chronic compartment syndrome, this results in pain, cramping, tingling and/or numbness during activities such as running. These sensations tend to go away once the activity has stopped, though the muscles in the area of the symptoms may feel tight.
The lower leg is divided into four compartments; anterior, lateral, posterior, and deep posterior. Each of these compartments contains several muscles, along with corresponding nervous tissue and blood vessels. The compartments are separated by fascia (thick layers of tissue) that to not stretch or expand easily. Therefore, when swelling occurs within a compartment, increased pressure can be placed on the muscles, capillaries and nerves. In the case of chronic compartment syndrome, this results in pain, cramping, tingling and/or numbness during activities such as running. These sensations tend to go away once the activity has stopped, though the muscles in the area of the symptoms may feel tight. 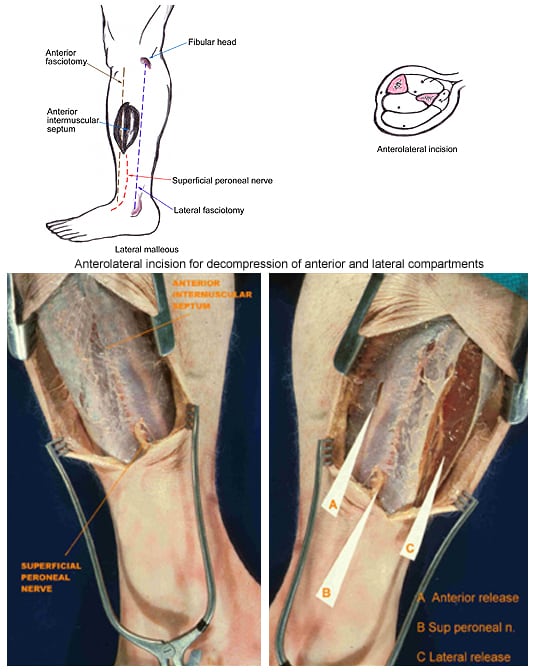 - Surgery: Unfortunately, surgical procedures seem to be the most effective treatment for chronic compartment syndrome. The most common surgery for compartment syndrome is a fasciotomy, or compartment release, which involves cutting the fascia to allow the muscle swell, and subsequently relieving the excess pressure. There are several techniques for performing this surgery, though the most common is the double-incision fasciotomy (shown on right). Rehabilitation is required after surgery, so compartment syndrome patients (especially athletes) should anticipate a fairly long recovery time before returning to normal activity.
- Surgery: Unfortunately, surgical procedures seem to be the most effective treatment for chronic compartment syndrome. The most common surgery for compartment syndrome is a fasciotomy, or compartment release, which involves cutting the fascia to allow the muscle swell, and subsequently relieving the excess pressure. There are several techniques for performing this surgery, though the most common is the double-incision fasciotomy (shown on right). Rehabilitation is required after surgery, so compartment syndrome patients (especially athletes) should anticipate a fairly long recovery time before returning to normal activity.